Chapter 13. The Urinary System
13.5 Physiology of Urine Formation: Tubular Reabsorption and Secretion
Learning Objectives
By the end of this section, you will be able to:
- state the areas of the nephron in which reabsorption of water and/or solutes occurs;
- define apical and basolateral sides of an epithelial cell;
- identify the PCT as the site where most tubular reabsorption occurs;
- state the approximate percentage of total filtrate reabsorbed per day;
- state the specific location of Na+/K+ ATPases in the PCT epithelium and diagram and explain the roles of the Na+/K+ATPases in the direct or indirect reabsorption of most substances by the PCT, including Na+, K+, water, glucose, amino acids, vitamins, and urea;
- explain the role of cotransport in the reabsorption of glucose, amino acids, and vitamins by the PCT;
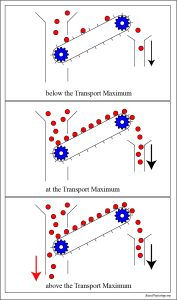
- define transport maximum (Tm) and how Tm for cotransporters in the PCT affects glucose reabsorption;
- explain, using the concept of Tm, how diabetes mellitus can lead to glycosuria;
- describe how filtrate osmolarity changes as the filtrate passes through the nephron;
- state the substances reabsorbed by the descending and ascending limbs of the loop of Henle;
- state the sites of production and release of aldosterone, ANP, PTH, and ADH;
- state the main regions of the nephron targeted by aldosterone, ANP, PTH, and ADH and explain the effects of each of these hormones on reabsorption and/or secretion of specific substances;
- state the role of PTH in activation of vitamin D; and
- state the areas of the nephron in which most secretion occurs.
Tubular Reabsorption and Secretion: Membrane Transport Mechanisms
Tubular reabsorption and secretion each involve transport of substances across plasma membranes. The membrane transport mechanisms utilized are simple diffusion, facilitated diffusion, osmosis, primary active transport, and cotransport (secondary active transport) (Table 13.2). Each of these is reviewed below. For a detailed explanation of each, visit Chapter 4.
In simple diffusion, a substance moves from a higher to a lower concentration down its concentration gradient, directly through the lipid bilayer of the plasma membrane. Simple diffusion is a type of passive transport: it requires no cellular energy. Osmosis is the diffusion of water across a semipermable membrane (in living systems, this is the plasma membrane); water moves from an area of lower solute concentration to an area of higher solute concentration, in other words from a more dilute solution to a less dilute solution.
Facilitated diffusion is similar to simple diffusion in that the substance moves down its concentration gradient. The difference is that facilitated diffusion requires specific membrane carrier proteins or protein channels for movement. For example, the Na+ and K+ leakage channels found in plasma membranes carry out facilitated diffusion: Na+ and K+ are moving down their gradients through the channels. Facilitated diffusion is passive; it requires no cellular energy.
Active transport mechanisms move substances across the plasma membrane against their gradients: from lower to higher concentration. Active transport requires energy. Primary active transport proteins (pumps) directly use the energy stored in the phosphate bonds in ATP: primary active transport proteins catalyze the hydrolysis of ATP to ADP and phosphate. The energy released in this reaction is used my primary active transport pumps to move substances against their gradients. An example of a primary active transport protein is the Na+/K+ pump (Na+/K+ ATPase). Secondary active transport, also called cotransport, uses energy stored in ion gradients to move substances against their gradients across the membrane. Cotransport always involves the movement of one substance (usually an ion) down its gradient and another substance against its gradient: the movement of the ion down its gradient releases energy that is used to move the other substance against its gradient. Recall from chapter 4 that a symport is a cotransporter that moves substances in the same direction across the membrane, while an antiport moves two substances in opposite directions across the membrane.
In addition to moving across the plasma membrane (the transcellular route), some substances move in between cells as they are reabsorbed. This route of movement is called the paracellular route (Figure 13.5.1). Figure 13.5.1 also reviews the polarity, or sidedness, found all in epithelial cells: epithelia possess an apical and a basolateral (basal) side. Regarding the nephron tubules, the apical side is the side facing the lumen of the tubule, and the basolateral (basal) side is the side facing the interstitial fluid and capillary bed.
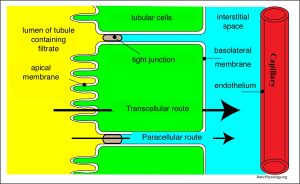
Table 13.2 summarizes the mechanisms by which substances are reabsorbed and secreted in different portions of the nephron.
| Substance | PCT | Loop of Henle | DCT | Collecting Ducts |
|---|---|---|---|---|
| Glucose | 100% reabsorbed; cotransport with Na+ | none | none | none |
| Amino acids | 100% reabsorbed; cotransport with Na+ | none | none | none |
| Vitamins | 100% reabsorbed; cotransport and primary active transport | none | none | none |
| Lactate | Majority reabsorbed; diffusion and potentially active transport | none | none | none |
| Creatinine | Secreted | none | none | none |
| Urea | 50% reabsorbed passively via a variety of mechanisms; also actively secreted | Reabsorption, facilitated diffusion in descending limb; secretion in ascending limb | none | Reabsorption in medullary collecting ducts; facilitated diffusion |
| Sodium | 65% reabsorbed via a variety of processes | 25% reabsorbed in thick ascending limb; active transport | actively reabsorbed; stimulated by aldosterone | actively reabsorbed, stimulated by aldosterone; reabsorption inhibited by ANP (atrial natriuretic peptide) |
| Chloride | 50% reabsorbed, cotransport with Na+, diffusion | Reabsorbed in thin and thick ascending limb; diffusion in ascending limb | Reabsorbed; diffusion | Reabsorbed; symport |
| Water | 65% reabsorbed osmotically with solutes | 15% reabsorbed in descending limb; osmosis | Variable amounts reabsorbed, controlled by ADH, osmosis | Variable amounts reabsorbed, controlled by ADH, osmosis |
| Bicarbonate (HCO3–) | 80% to 90% reabsorption; cotransport with Na+; coupled with H+ secretion | Reabsorbed, cotransport (symport with Na+ and antiport with Cl–) in ascending limb | none | Reabsorbed; cotransport with Cl– |
| H+ | Secreted; cotransport with Na+; coupled with HCO3– reabsorption | none | Secreted; active | Secreted; active |
| NH4+ | Secreted; diffusion | none | Secreted; diffusion | Secreted; diffusion |
| Certain drugs | Secreted; active transport | none | Secreted; active | Secreted; active |
| K+ | 65% reabsorbed; diffusion | 20% reabsorbed in thick ascending limb; symport | Secretion controlled by aldosterone; active | Secretion controlled by aldosterone; active |
| Ca++ | 60% to 70% reabsorbed; mainly paracellular | 25% reabsorbed in thick ascending limb; diffusion and paracellular | up to 8% reabsorbed; controlled by PTH (parathyroid hormone); facilitated diffusion | Minimal to no reabsorption |
| Mg++ | Reabsorbed; diffusion | Reabsorbed in thick ascending limb; diffusion | Reabsorbed | none |
| HPO4++ | Reabsorbed, inhibited by PTH (parathyroid hormone), diffusion | none | Reabsorbed; diffusion | none |
Tubular Reabsorption
As previously mentioned, up to 180 L of filtrate is formed per day by the nephrons, and approximately 99% of that filtrate is reabsorbed, resulting in about 1 to 2 L urine formed/day. Reabsorption is essential to reclaim substances from the filtrate that the body needs and to prevent their excretion.
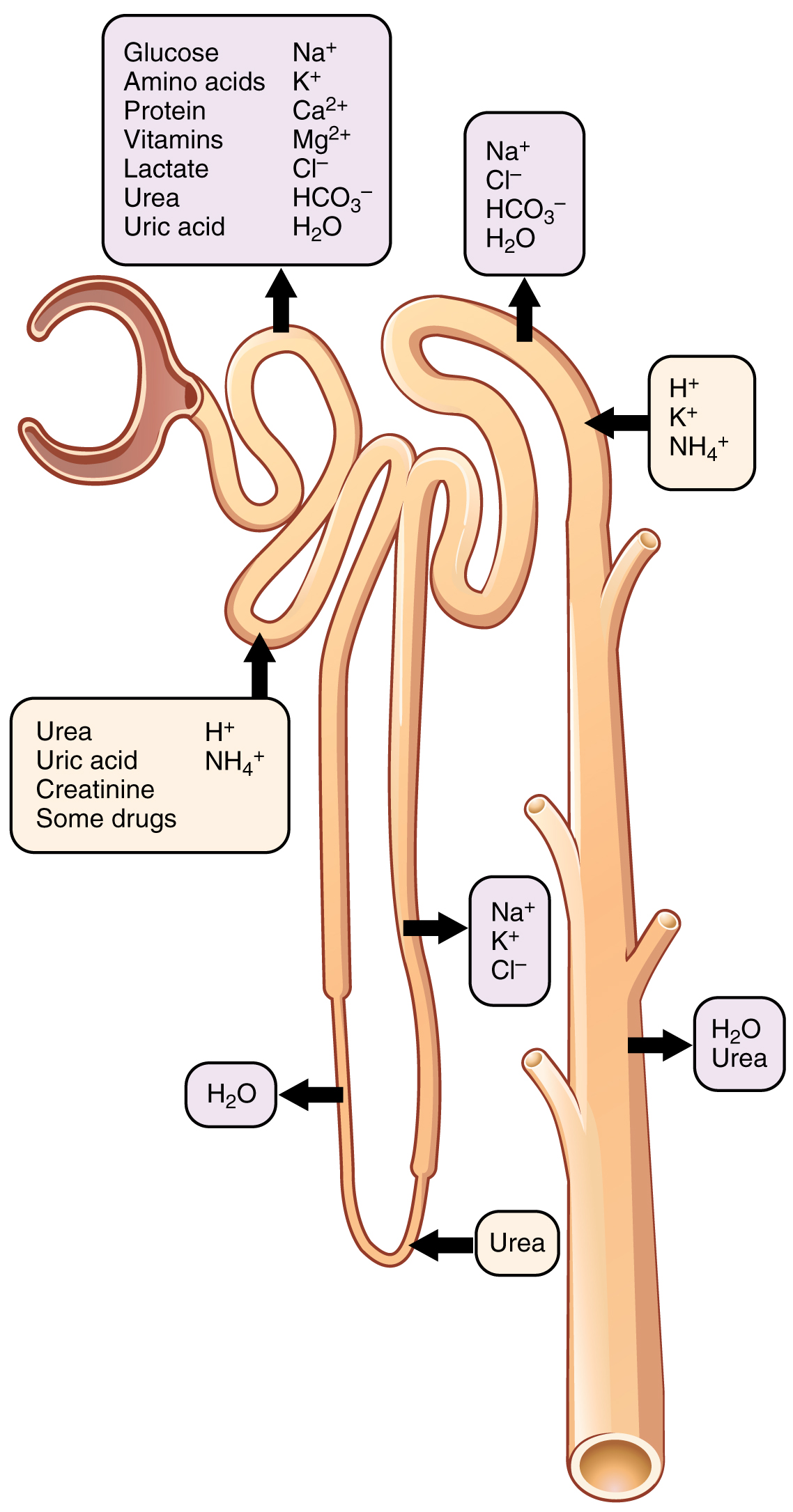
Various portions of the nephron differ in their capacity to reabsorb water and specific solutes (Table 13.2 and Figure 13.5.2).
Reabsorption in the Proximal Convoluted Tubule
| Substance Reabsorbed (Amount Reabsorbed from Filtrate) | Mechanism |
|---|---|
| Na+ (65%) | primary active transport via Na+/K+ ATPases on basolateral side; cotransport on apical side |
| Nutrients (glucose, amino acids, vitamins) (100%) | Cotransport with Na+ |
| Cl– (50%)
K+ (65%) Ca++ (60% to 70%) Mg++ (variable) |
passive; paracellular route |
| Water (65%) | osmosis; driven by solute reabsorption (obligatory water reabsorption) |
| lipid soluble solutes (variable) | diffusion driven by concentration gradient created by water reabsorption |
| HCO3– (80% to 90%) | cotransport with Na+; coupled with H+ secretion |
| Urea (50%) | passive; mainly paracellular route |
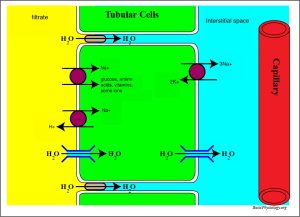
About 65% of the Na+ entering the nephron is reabsorbed in the PCT and returned to the circulation. Na+ is reabsorbed by the PCT via a variety of transport mechanisms, including active transport via activity of Na+/K+ ATPases on the basolateral side (Figure 13.5.3). The activity of the Na+/K+ pumps drives the reabsorption of many other substances by the PCT. The Na+/K+ pumps create concentration gradients that drive:
- reabsorption of 100% of amino acids and glucose in the filtrate via cotransport with Na+;
- reabsorption of more Na+ via a Na+/H+ antiport;
- reabsorption of 65% of water in the filtrate via osmosis through aquaporins; this is obligatory water reabsorption, water reabsorption that occurs due to solute reabsorption: water is “obliged” to follow the solutes regardless of the body’s hydration state. This water movement out of the filtrate increases the concentration of solutes still in the filtrate, which then leads to their passive reabsorption. This includes:
- reabsorption of ions such as Cl–, K+, Mg++, and Ca++ mainly via paracellular route;
- reabsorption of 80% to 90% of HCO3– in the filtrate via cotransport with Na+;*
- reabsorption of lipid-soluble substances by the transcellular route; and
- reabsorption of urea via the paracellular route.**
* Bicarbonate reabsorption is coupled to H+ secretion and is extremely important in maintaining acid-base balance in the body. This is discussed in detail in Chapter 14.
** Although urea is a nitrogenous waste, 50% of filtrate urea is reabsorbed by the PCT. Urea will be discussed in a later section of this chapter.
Reabsorption in the Loop of Henle
The loops of Henle of cortical nephrons do not extend into the renal medulla very far, if at all. Juxtamedullary nephrons have loops that extend variable distances, some very deep into the medulla. The descending and ascending limbs of the loop differ in their permeability to salt and to water, as discussed next. Solutes and water reabsorbed from the filtrate in the loop of Henle are returned to the circulation by way of the peritubular capillaries (cortical nephrons) or vasa recta (juxtamedullary nephrons.)
Descending Limb of the Loop of Henle
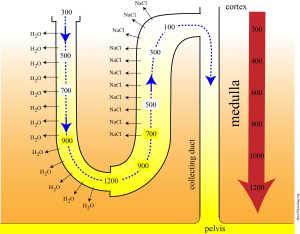
About 15% of the water in the filtrate is reabsorbed by the descending limb. Virtually no solutes are reabsorbed here. Plasma membranes in the descending limb have permanent aquaporins that allow obligatory water reabsorption out of the descending limb into the surrounding interstitial fluid. The interstitial fluid osmolarity in the kidney increases in concentration from the cortex to the medulla (Figure 13.5.5.) This vertical osmotic gradient in the interstitium is what causes water to move passively out of the descending limb. (It then enters the vasa recta).
As water is reabsorbed from the filtrate, filtrate osmolarity increases from about 300 mOsm to about 1200 mOsm at the hairpin turn of the longest loops of Henle.
About 80% of the solutes that were filtered in the glomerulus have now been recovered along with a majority of the water in the filtrate. As the filtrate enters the ascending loop, the permeability of the cells of the loop changes significantly.
Ascending Limb of the Loop of Henle
The ascending limb is not permeable to water; no water reabsorption occurs here. As seen in figure 13.5.6, NaCl is reabsorbed here. It is important to note that other solutes are reabsorbed by the ascending limb as well, but by convention many texts just show NaCl for clarity. Solute reabsorption occurs via active transport processes. The main transporter is a Na+-K+-2Cl cotransporter in the apical membrane, often abbreviated NKCC2. This symport is essential for reabsorption Na+, Cl-, and K+ from the filtrate. The reabsorption of of solutes, but not water, results in a filtrate that is relatively dilute (about 100 Osm) by the time is reaches the DCT.
Reabsorption in the Distal Convoluted Tubule and Collecting Duct
Approximately 80% of filtered water has been recovered by the time the dilute filtrate enters the DCT. Under hormonal action, additional water and solutes can be reabsorbed from the DCT and collecting duct and returned to the circulation.
PTH, Calcium Reabsorption by the DCT, and Calcitriol Formation
Ca++ reabsorption from the filtrate in the DCT is controlled by parathyroid hormone (PTH) released by the parathyroid glands. As PTH levels increase, Ca++ reabsorption increases.
PTH also stimulates the kidneys to convert vitamin D into its active form, calcitriol. Once vitamin D is produced by the skin or obtained via dietary sources, it is converted into 25-hydroxy vitamin D by the liver. PTH then stimulates the kidneys (mainly the PCT) to convert 25-hydroxy vitamin D into calcitriol. Calcitriol is essential for intestinal absorption of dietary calcium.
Aldosterone, Atrial Natriuretic Peptide (ANP), and Sodium Reabsorption by the DCT and Collecting Duct
Na+ reabsorption from the filtrate in the DCT and collecting duct is controlled by aldosterone, a hormone release by the adrenal cortex. Aldosterone is discussed in more detail in this chapter in Section 13.4. As aldosterone levels increase, Na+ reabsorption from the filtrate increases.
Atrial natriuretic peptide (ANP) is a hormone released by the atria. In response to increased stretch, the atria release ANP. ANP has an effect opposite of aldosterone: as ANP levels increase, Na+ reabsorption from the filtrate decreases. ANP acts mainly on the collecting duct.
Antidiuretic Hormone (ADH) and Water Reabsorption by the DCT and Collecting Duct
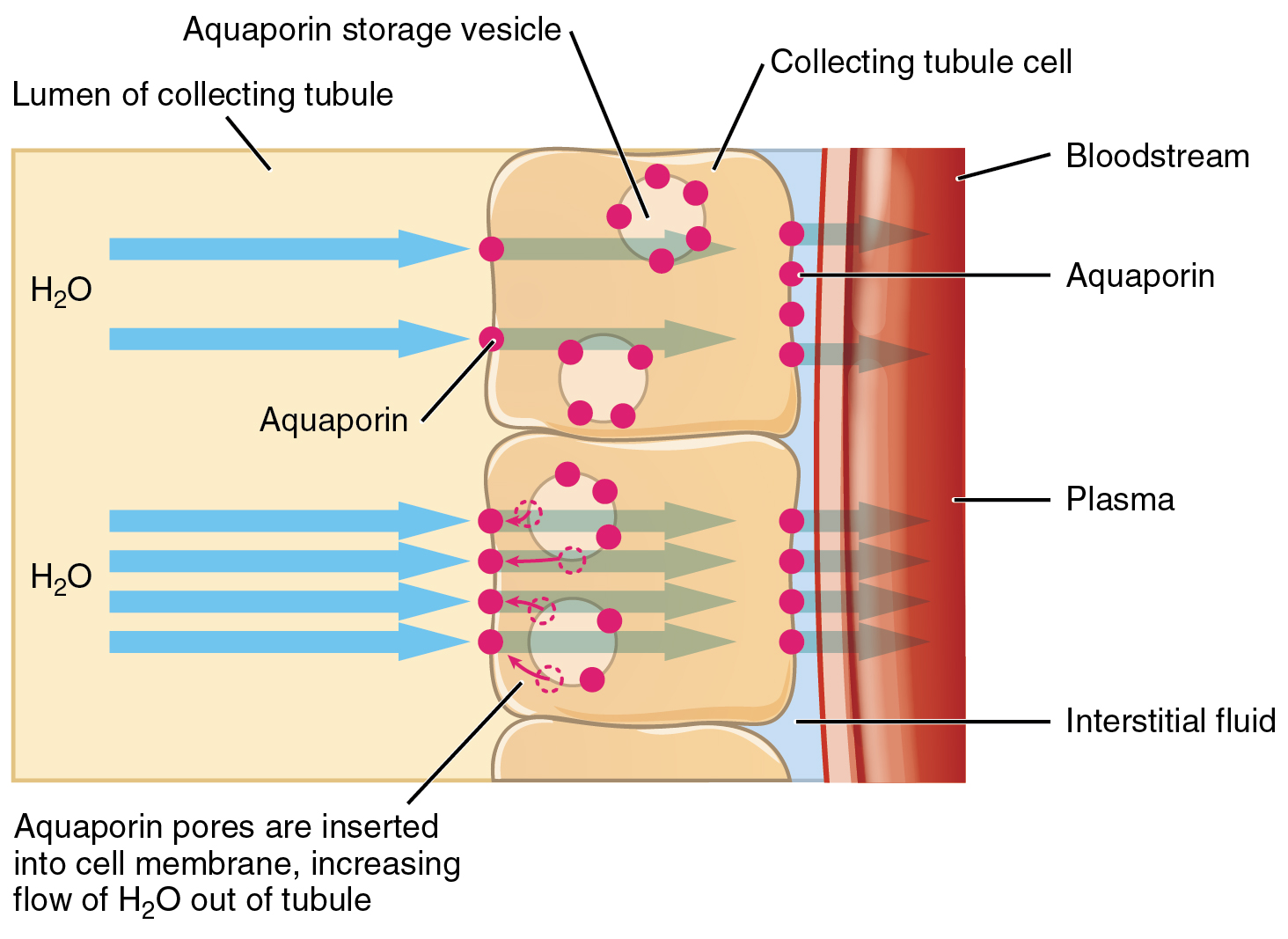
ADH is produced by the hypothalamus and released by the posterior pituitary. Without sufficient ADH, the DCT and collecting duct are nearly impermeable to water. In response to various stimuli, ADH levels increase, which causes the principal cells of the late DCT and the collecting duct to insert water channel proteins called aquaporins into their apical surface (Figure 13.5.6). The result is an increase in the water permeability of these cells and therefore an increase in water reabsorption from the filtrate into the blood. This results in the excretion of a more concentrated urine. When levels of ADH decrease, aquaporins are removed from the tubule cell apical membranes, and the reabsorption of water out of the filtrate decreases, resulting in the excretion of more dilute urine.
Adjustable water reabsorption according to ADH is called facultative water reabsorption.
Tubular Secretion
Tubular secretion occurs mostly in the PCT and DCT where substances are moved from the peritubular capillaries into the lumen of the tubule. Secretion usually removes substances that are too large to be filtered (for example: antibiotics, toxins, and food additives) or those that are in excess in the blood (for example, H+ and K+).
Secretion of K+ by the DCT (and the collecting duct) is under the control of aldosterone: as aldosterone levels increase, K+ secretion increases. Secretion of H+ is an important mechanism by which kidneys maintain acid-base balance, discussed further in Chapter 14.
Section Review
Tubular reabsorption and secretion each involve transport of substances across plasma membranes. The membrane transport mechanisms utilized are simple diffusion, facilitated diffusion, osmosis, primary active transport, and cotransport.
Most reabsorption occurs in the PCT: 100% of glucose, amino acids, and vitamins in the filtrate are reabsorbed here, along with 65% of Na+ and water and 80% to 90% of the bicarbonate in the filtrate, among other substances. The descending limb of the loop of Henle reabsorbs water but not solutes, while the ascending limb reabsorbs solutes (mainly NaCl) but not water. Reabsorption of substances including Na+, Ca++, and water in the DCT and collecting duct varies according to the levels of the hormones aldosterone and ANP (Na+), PTH (Ca++), and ADH (water.)
The main areas of the nephron in which secretion occurs are the PCT and DCT, with some also occurring in the collecting duct. Secretion of K+ by the DCT and the collecting duct is controlled by aldosterone.
Review Questions
Critical Thinking Questions
Glossary
- aldosterone
- hormone released by the adrenal cortex that stimulates Na+ reabsorption by the DCT and collecting duct
- antidiuretic hormone (ADH)
- hormone that stimulates water reabsorption by the DCT and collecting duct
- atrial natriuretic peptide (ANP)
- hormone released by the atria that stimulates a decrease in Na+ reabsorption by the collecting duct
- cotransport
- membrane transport mechanism that uses the energy stored in ion gradients to move substances across the plasma membrane against their gradients; one substance is moving down its gradient while another is moving against its gradient; also called secondary active transport.
- facultative water reabsorption
- adjustable water reabsorption in response to ADH levels
- glycosuria
- presence of glucose in the urine; caused by high blood glucose levels that exceed the ability of the kidneys to reabsorb the glucose; usually the result of untreated or poorly controlled diabetes mellitus
- obligatory water reabsorption
- water reabsorption due to solute reabsorption; water follows salt movement down an osmotic gradient
- parathyroid hormone (PTH)
- hormone that stimulates calcium reabsorption by the DCT; released by parathyroid glands
- vertical osmotic gradient
- increase in osmolarity of the interstitial fluid in the kidney from the cortex to the medulla
Glossary Flashcards
References
Lammers, W. (2025). Loop of Henle. BasicPhysiology.org – A simple website to teach human physiology. (Accessed May 2025).
Lammers, W. (2025). The proximal convoluted tubule. BasicPhysiology.org – A simple website to teach human physiology. (Accessed May 2025).
This work, Human Physiology, is adapted from Anatomy & Physiology by OpenStax, licensed under CC BY. This edition, with revised content and artwork, is licensed under CC BY-SA except where otherwise noted.
Images from Anatomy & Physiology by OpenStax are licensed under CC BY except where otherwise noted.
Access the original for free at OpenStax.
Report an Error
Did you find an error, typo, broken link, or other problem in the text? Please follow this link to the error reporting form to submit an error report to the authors.
