Chapter 13. The Urinary System
13.6 Physiology of Urine Formation: The Vertical Osmotic Gradient and Altering Urine Concentration
Learning Objectives
- explain the role of the loop of Henle as a countercurrent multiplier in establishing the vertical osmotic gradient in the kidney interstitial fluid;
- explain the role of the vasa recta as a countercurrent exchanger in maintaining the vertical osmotic gradient in the kidney interstitial fluid;
- state the two main substances found in the medullary interstitial fluid that contribute to the vertical osmotic gradient;
- describe the effect of ADH on final urine concentration by explaining ADH effects on the distal nephron; and
- describe the importance of the vertical osmotic gradient to the kidneys’ ability to excrete concentrated urine.
As described earlier, filtrate is the fluid that results from filtration of the plasma into the glomerular capsule. Urine is the waste product resulting from the processing of filtrate: once the filtrate has passed through the entirety of the nephron and exits the collecting ducts, it is called urine. Normally, the kidneys excrete an average of 800 to 2,000 mL of urine per day, but the volume of urine excreted varies depending on several factors. For example, the food and liquids ingested by a person and their hydration status affect urine output. Additionally, certain medications alter the volume of urine produced.
As mentioned in Section 13.0, one of the main functions of the kidneys is osmoregulation, which is maintaining the osmolarity (solute concentration) of the blood. The kidneys maintain plasma solute concentration by varying urine concentration and volume. The concentration of urine produced varies throughout a day depending on the body’s needs. To understand this, consider these extremes:
- when a person is dehydrated and water needs to be conserved, the kidneys produce a small volume of concentrated urine; and
- when a person is overhydrated and excess water needs to be excreted, the kidneys produce a large volume of dilute urine.
The kidneys’ ability to vary urine concentration and volume relies on the vertical osmotic gradient in the interstitial fluid of the kidney (Figure 13.6.1.)
Countercurrent Mechanisms and Establishment of the Vertical Osmotic Gradient
The vertical osmotic gradient of the interstitial fluid of the kidney is created and maintained countercurrent mechanisms occurring in the Loops of Henle and the vasa recta of juxtamedullary nephrons. The term “countercurrent” refers to opposite fluid flow in adjacent tubes. Two countercurrent systems function in the nephron:
- the countercurrent multiplier system of the Loops of Henle of juxtamedullary nephrons; and
- the countercurrent exchanger system of the vasa recta surrounding the Loops of Henle.
Countercurrent Multiplier System: Establishment of the Vertical Gradient
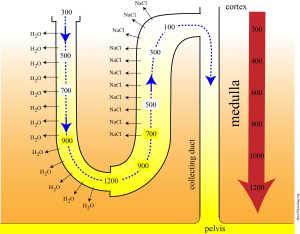
The longer loops of Henle of juxtamedullary nephrons are countercurrent multipliers. “Countercurrent” refers to the opposite flow of filtrate in the descending and ascending limbs (Figure 13.6.1). “Multiplier” refers to the fact that the osmolarity of the interstitial fluid is multiplied, or increased, as we move from the cortex into the medulla (Figure 13.6.1). This multiplication results from the countercurrent flow of filtrate and the different permeabilities of the descending and ascending limbs. Remember that the descending limb is permeable to water, but not salts, and the ascending limb is permeable to salts, but not water.
The ascending limb actively pumps out salts, mainly NaCl, which adds to the osmolarity of the interstitial fluid. The countercurrent flow in and the different properties of the descending and ascending limbs establish a positive feedback cycle by which this pumping action of the ascending limb is multiplied. The cycle can be summarized as follows:
- the ascending limb pumps NaCl out of the filtrate, which increases the interstitial fluid osmolarity;
- the increased interstitial fluid osmolarity causes water to move out of the descending limb via osmosis; and
- as water leaves the filtrate in the descending limb, its concentration increases, providing salt to be pumped out of the ascending limb (back to step 1).
External Website
Watch this video to help you visualize the role of the loop of Henle as countercurrent multiplier. Click here to view “Loop of Henle Explained” by Biomed Sessions (July 3, 2014) in a separate tab.
Urea Recycling and the Vertical Osmotic Gradient
The countercurrent multiplication carried out by the loop of Henle adds NaCl to the interstitial fluid, increasing its osmolarity. NaCl is not the only solute causing this increased osmolarity, however. Urea is also present in the interstitial fluid and contributes to the vertical osmotic gradient. This can be confusing, since urea is a metabolic waste product. Indeed, about 40% to 50% of the urea in the filtrate is eventually excreted in the urine. However, the presence of urea in the interstitial fluid is vital to increasing the osmolarity of the interstitial fluid.
The handling of urea by the nephron is complicated, but here we focus on how urea is added to the interstitial fluid. This is accomplished via the “recycling” of urea between the collecting duct filtrate, the interstitial fluid of the medulla, and the filtrate in the ascending limb (Figure 13.6.2).

Countercurrent Exchanger System: Maintenance of the Vertical Gradient
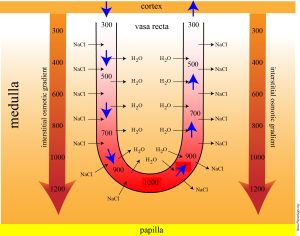
The vasa recta surrounding the loop of Henle functions as a countercurrent exchanger: the flow of blood in the two limbs of the vasa recta is countercurrent and as seen in Figure 13.6.3, the blood flowing through the vasa recta equilibrates with surrounding interstitial fluid. This countercurrent arrangement of flow is important in preventing rapid removal of NaCl from the interstitial fluid and in reabsorbing water. In general, blood flows slowly in capillaries to allow time for exchange of nutrients and wastes. In the vasa recta particularly, this rate of flow is important for two additional reasons. The flow must be slow to allow blood cells to lose and regain water without either crenating or bursting. Second, a rapid flow would remove too much Na+ and urea, destroying the osmotic gradient. As the vasa recta descends, Na+ and urea are freely able to enter the capillary, while water freely leaves; as they ascend, Na+ and urea leave the filtrate into the surrounding medulla, while water reenters the blood.
-
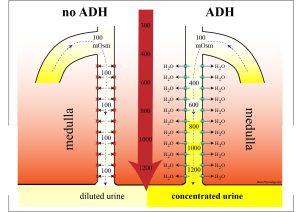
- if the blood becomes hyperosmotic, ADH levels increase and more water is reabsorbed and a smaller volume of concentrated urine is excreted;
- if the blood becomes hyposmotic, ADH levels decrease and less water is reabsorbed and a larger volume of dilute urine is excreted.
Section Review
The kidneys maintain plasma solute concentration by varying urine concentration and volume. Their ability to excrete concentrated urine depends on the presence of the vertical osmotic gradient in the interstitial fluid of the kidney. The vertical osmotic gradient is established by the countercurrent multiplier mechanism of the loops of Henle of juxtamedullary nephrons: the ascending limb pumps NaCl into the medullary interstitial fluid, which contributes to the increased osmolarity here. Urea also accumulates in the interstitium due to urea recycling. The vasa recta is a countercurrent exchanger that maintains the vertical osmotic gradient.
ADH is a signal that water needs to be conserved: as ADH levels rise in response to various stimuli, the permeabilities of the DCT and collecting duct to water increases and water is reabsorbed. This results in the excretion of a smaller volume of concentrated urine. When ADH levels are low, a larger volume of dilute urine is excreted.
Review Questions
Critical Thinking Questions
Glossary
- countercurrent exchange
- mechanism by which vasa recta maintains the vertical osmotic gradient; involves the vasa recta equilibrating with the surrounding interstitial fluid
- countercurrent multiplication
- mechanism by which the ascending and descending limbs of the loop of Henle establish the vertical osmotic gradient; involves pumping of NaCl into the interstitial fluid
- filtrate
- fluid produced by filtration of plasma into the glomerular capsule
- osmoregulation
- maintaining the solute concentration of the blood
- urine
- waste product formed from processing of the filtrate by the nephron; transported from the kidneys to the bladder via the ureters
Glossary Flashcards
References
Lammers, W. (2025). Loop of Henle. BasicPhysiology.org – A simple website to teach human physiology. (Accessed May 2025).
Lammers, W. (2025). The collecting ducts. BasicPhysiology.org – A simple website to teach human physiology. (Accessed May 2025).
This work, Human Physiology, is adapted from Anatomy & Physiology by OpenStax, licensed under CC BY. This edition, with revised content and artwork, is licensed under CC BY-SA except where otherwise noted.
Images from Anatomy & Physiology by OpenStax are licensed under CC BY except where otherwise noted.
Access the original for free at OpenStax.
Report an Error
Did you find an error, typo, broken link, or other problem in the text? Please follow this link to the error reporting form to submit an error report to the authors.
